These meal prep recipes are the healthy, practical recipes I return to when I want weekday breakfasts, lunches, dinners, and snacks handled before the week gets busy. I selected these healthy meal prep recipes because they bring a satisfying balance of protein, fiber-rich ingredients, and produce, while still making sense to store, pack, reheat, or freeze.
Jump to:
Start here: For five weekday lunches, pick one portion-ready lunch plus one flexible component. For variety all week, add a breakfast and a freezer backup instead of making five identical containers.
Why You’ll Love These Meal Prep Recipes
Actually practical: I chose easy meal prep recipes that can be portioned, packed, refrigerated, frozen, or repurposed without turning into disappointing leftovers.
A plan for every meal: This list covers grab-and-go breakfasts, cold lunches, reheat-friendly dinners, snacks, and flexible building blocks.
Tested Fit Foodie Finds recipes: As a recipe developer and food photographer, I chose recipes I would genuinely make again after the first cook.
Healthy without being restrictive: I lean into protein, fiber, produce, and familiar flavors rather than rigid rules.
How to Choose the Right Meal Prep Style
Before choosing meal prep recipes, use this quick decision guide. It is especially helpful for meal prep for beginners because meal prep does not need to mean eating the same container five days in a row.
Style
Best for
How I use it
Portion-ready meals:
Grab-and-go lunches
Choose bowls, bakes, salads, and soups that are ready to pack.
Prep-once components:
More variety
Mix a protein, grain or legume, vegetables, and sauce in different combinations.
Freezer backup:
Busy weeks
Keep burritos, breakfast items, soups, or baked portions ready for later.
For flexible lunches, pair a protein and grain with a sturdy salad or one of my favorite healthy salad ideas.
Meal Prep Breakfast Recipes
Choose breakfasts that are portable, protein-aware, or freezer-friendly so mornings require less decision-making. These healthy meal prep recipes make the first meal of the day feel much more doable.
Breakfast Burritos (Make-Ahead or Fresh)
These burritos make a hearty morning option with a make-ahead filling and a handheld format. Prep label: Freeze individually or refrigerate for quick reheating.
Bacon, Egg, and Cheese Breakfast Burritos
This bacon, egg, and cheese version is a satisfying freezer-focused breakfast I reach for on rushed mornings. Prep label: Freeze wrapped burritos; reheat one at a time.
A dump-and-bake casserole gives me a savory breakfast that can be sliced into convenient portions. Prep label: Refrigerate portions and warm before serving.
Baked oatmeal cups are naturally portable and easy to portion for the week. Prep label: Refrigerate for grab-and-go mornings or freeze extras.
Quick & Easy Baked Eggs (Perfect for Meal Prep)
A batch of baked eggs is a simple savory base for breakfast boxes, toast, or grain bowls. Prep label: Refrigerate portions and reheat as needed.
Brown Sugar Shaken Espresso Overnight Oats (Starbucks Inspired!)
Overnight oats deliver a creamy, coffee-shop-inspired breakfast without morning cooking. Prep label: Refrigerate in individual jars and eat chilled.
Sheet Pan Protein Pancakes (14g Protein per Serving!)
Sheet pan protein pancakes turn a favorite breakfast into easy, evenly portioned squares. Prep label: Refrigerate slices and reheat or enjoy cold.
Healthy Apple Muffins with Cottage Cheese (High Protein!)
These cottage cheese apple muffins bring a high-protein option to the breakfast rotation. Prep label: Store chilled for the week or freeze a portion for later.
Protein Lemon Cream Pie Chia Seed Pudding
This lemon cream chia pudding is a bright, protein-forward breakfast or snack that is ready when I am. Prep label: Refrigerate in covered single servings and eat chilled.
The Best Protein Breakfast Smoothie
A protein smoothie is an easy option when I want a quick breakfast with fruit and staying power. Prep label: Blend fresh, or prep the ingredients ahead for a fast morning smoothie.
Meal Prep Lunch Recipes
Lunch is often the biggest weekday pain point, so I look for meals that travel well, keep their texture, and feel satisfying enough to carry me through the afternoon. These meal prep recipes layer protein, fiber-rich carbohydrates, produce, and big flavor without prescribing a calorie target.
Cold lunches, salads, and mason jars: Pack dressings and crisp toppings separately whenever the individual recipe calls for it.
Dill Pickle White Bean Salad
Creamy white beans and dill pickle flavor make this a sturdy, protein- and fiber-aware lunch that does not rely on delicate greens. Prep label: Refrigerate in covered containers and serve chilled.
Make-Ahead Taco Salad
This taco salad is a component-packed option that makes lunch feel far from boring. Prep label: Store crunchy toppings and dressing separately, then assemble when ready.
Tex Mex Quinoa Mason Jar Salad
Layered quinoa and Tex-Mex ingredients make this mason jar salad especially convenient for weekday packing. Prep label: Refrigerate in jars; keep the layers intact until serving.
Thai Chicken Salad
A Thai chicken salad gives me a protein-led cold lunch with fresh flavor and satisfying texture. Prep label: Refrigerate the salad; add dressing or crunchy toppings at serving.
Herby Cucumber Tomato Salad
Herby cucumber and tomato make a fresh, simple side for a cold lunch box or component-style meal. Prep label: Refrigerate covered and serve chilled.
Mexican Quinoa Salad
This Mexican quinoa salad is a colorful make-ahead option built around sturdy grains, beans, and vegetables. Prep label: Refrigerate for a cold, packable lunch.
Easy Chickpea Salad
Chickpea salad is a versatile, plant-forward filling for lettuce cups, sandwiches, or a snacky lunch plate. Prep label: Refrigerate covered and scoop into lunches through the week.
Bowls, bakes, and warm lunches: These easy meal prep recipes are designed to portion well or let you keep components separate until lunch.
These Philly cheese steak bowls are specifically built for meal prep, with a protein-and-vegetable base that feels substantial. Prep label: Portion into containers and reheat for lunch.
A one-pan chicken enchilada casserole brings rice, chicken, and bold flavor together for a dependable warm lunch. Prep label: Refrigerate individual portions and reheat.
Spinach Quinoa Lasagna Casserole
This spinach quinoa lasagna casserole is a vegetarian-friendly option for a cozy, portionable lunch. Prep label: Refrigerate slices and warm before eating.
5-Star, Award-Winning Beef Chili
A pot of beef chili gives me a filling lunch that is easy to divide into individual servings. Prep label: Refrigerate portions or freeze extras for later.
High Protein Creamy Chicken Soup
Creamy chicken soup adds a comforting, protein-forward option to a lunch plan. Prep label: Refrigerate in single servings and reheat gently.
Crispy Air Fryer Fried Rice
Air fryer fried rice is a flexible way to turn rice and vegetables into a warm lunch bowl. Prep label: Refrigerate portions and reheat before serving.
Vibrant Falafel Bowls with Turmeric Rice
Falafel bowls with turmeric rice offer a colorful vegetarian lunch with plenty of components. Prep label: Store the rice, falafel, and fresh toppings separately for best texture.
Meal Prep Dinner Recipes
These healthy meal prep recipes lower the weekday dinner load with bakes, soups, skillet meals, and simple proteins I can portion for reheating or pair with fresh sides.
Mediterranean Salmon Meal Prep
This salmon-centered meal prep brings seafood into the mix with Mediterranean flavors and satisfying components. Prep label: Refrigerate prepared portions and enjoy as a ready-to-go meal.
Mexican Stuffed Peppers
Mexican stuffed peppers make a colorful all-in-one dinner with built-in portions. Prep label: Refrigerate individual peppers and reheat for dinner.
Easy Stuffed Peppers
Classic stuffed peppers are a dependable make-ahead dinner when I want a protein, vegetable, and grain in one dish. Prep label: Portion and reheat leftovers for another meal.
Easy Honey Garlic Chicken
Honey garlic chicken is an easy protein to pair with rice and vegetables in different bowls through the week. Prep label: Refrigerate the chicken and reheat when assembling dinner.
Mexican Ground Beef Skillet
This Mexican ground beef skillet is a fast, flexible base for bowls, tacos, or salads. Prep label: Refrigerate the skillet mixture and reheat before serving.
Easy Chicken Tinga (Smoky & Perfectly Saucy)
Chicken tinga has saucy, bold flavor that works in tacos, bowls, and salads without feeling repetitive. Prep label: Refrigerate the filling and reheat in portions.
Salmon Noodle Casserole (with Chili Crunch & Boursin!)
A salmon noodle casserole is a cozy bake that turns into neat next-day dinner portions. Prep label: Refrigerate portions and reheat before eating.
Butter chicken meatballs offer a comforting dinner with a change of pace from plain chicken breast. Prep label: Refrigerate with sauce and reheat for an easy dinner.
Baked Street Corn Pasta
Baked street corn pasta is a crowd-pleasing casserole-style dinner that works well for dinner plus next-day lunch. Prep label: Portion into containers and reheat.
The Best Broiled Salmon (Simple Seasoning, 8 Min Broil!)
Broiled salmon cooks quickly, then becomes a versatile protein for dinner bowls or salads. Prep label: Refrigerate cooked salmon and add to meals through the week.
One-Pan Orzo and Chicken Sausage
One-pan orzo and chicken sausage gives me a complete skillet-style dinner with very little assembling. Prep label: Refrigerate portions and reheat for a weeknight dinner.
Hot Honey Shrimp Bowls
Hot honey shrimp bowls add seafood variety and a spicy-sweet flavor profile to the dinner lineup. Prep label: Store the bowl components separately, then reheat the shrimp and grain.
Meal Prep Snacks and Sweet Treats
These meal prep ideas make snacks easier to grab when I am hungry between meals; they are meant to reduce friction, not replace a full meal.
No-Bake Protein Bites (2 Ways: Thin Mint & S’mores)
These no-bake protein bites are a fun, portionable snack option with two flavor directions. Prep label: Refrigerate in a covered container for easy grab-and-go bites.
Birthday Cake Protein Balls (No Food Processor!)
Birthday cake protein balls bring a playful, protein-forward option to a snack box. Prep label: Refrigerate prepared balls in a covered container.
Peanut Butter Protein Balls (No Food Processor!)
Peanut butter protein balls are a classic, satisfying snack that needs no food processor. Prep label: Store chilled and portion a few for the day.
Homemade Peanut Butter Chocolate Chip Larabars
Homemade peanut butter chocolate chip bars are ideal when I want a portable, sweet snack made ahead. Prep label: Keep in a covered container; pack individual bars for later.
Peanut Butter Frozen Yogurt Bites
Frozen yogurt bites offer a cool, bite-size snack with a little peanut butter satisfaction. Prep label: Keep frozen and take out a few at a time.
Sweet Potato Hummus Recipe
Sweet potato hummus is a flavorful dip to pair with cut vegetables, crackers, or a wrap. Prep label: Refrigerate in a covered container and pack with produce separately.
Cottage Cheese Cookie Dough (No Protein Powder!)
Cottage cheese cookie dough is a high-protein sweet treat that feels special without a full baking project. Prep label: Refrigerate in covered portions and serve chilled.
Buffalo Chicken Protein Bars (Crispy + Baked)
Buffalo chicken protein bars make a savory alternative when I want a protein-focused snack beyond sweets. Prep label: Refrigerate portions and pack for a savory snack.
Freezer-Friendly Meal Prep Recipes
For weekly meal prep, I like to make a double batch when I have time, eat one batch this week, and keep the other as a realistic future-me backup—not an all-day mega-prep requirement.
Freezer note: Check the storage guidance on each individual recipe before freezing or reheating; freezer time and method are recipe-specific.
Build-Your-Own Meal Prep Components
These meal prep ideas give me more flexibility than identical containers. Prep a few parts once, then combine them differently across the week—especially helpful when people at the table have different tastes.
Greek Salad Recipe
Greek salad is a crisp, colorful side that brings vegetables and briny flavor to lunch boxes or dinner plates. Prep label: Refrigerate the salad and add delicate toppings when serving.
Fresh Caprese Quinoa Salad (15g Protein!)
This caprese quinoa salad is a grain-and-protein-forward component that is easy to spoon alongside a simple protein. Prep label: Refrigerate for a sturdy, cold side or lunch base.
The Best No Lettuce Salad
A no lettuce salad is a practical alternative when I want a make-ahead salad without delicate greens. Prep label: Refrigerate covered and serve chilled.
Juicy Air Fryer Chicken Breast (Ready in 20 Minutes)
Air fryer chicken breast is a versatile protein I can slice into bowls, salads, wraps, and grain plates. Prep label: Refrigerate cooked portions and reheat or serve cold.
How to Cook Perfect Quinoa
Perfectly cooked quinoa is an easy grain base for changing up bowls and salads all week. Prep label: Refrigerate in a covered container and add to meals as needed.
Easy Rainbow Grilled Vegetables
Rainbow grilled vegetables add color and produce to almost any protein-and-grain combination. Prep label: Refrigerate cooked vegetables and reheat or serve at room temperature.
A small set of components turns one prep session into many combinations, which is why these meal prep recipes can feel fresh beyond day one.
My Best Meal Prep Tips
These are my practical meal prep for beginners tips for making the list work in real life. Successful prep is about consistency and enjoyment, not rigidity.
Start smaller: Pick two or three recipes, not an aspirational 10-recipe marathon.
Build a mix: Choose one portion-ready meal, one flexible component recipe, and one freezer backup.
Match the container: Use containers that work for cold meals, reheating, or later assembly; keep dressings and crunchy toppings separate when called for.
Protect texture: Add contrast with a sauce, crunchy topping, fresh herb, or crisp vegetable so food stays enjoyable by day three.
Label freezer portions: Add the recipe name and date, then follow the storage guidance on that recipe.
Choose what you will want to eat: A realistic plan is always more useful than a perfect-looking one.
Meal Prep Recipes FAQs
What are the best meal prep recipes for the week?
The best meal prep recipes are the ones that fit your schedule and still taste good after they are stored. I recommend choosing a mix of a portion-ready lunch or dinner, a breakfast you can grab quickly, and a freezer-friendly option for busy days. Recipes with a protein source, fiber-rich carbs, vegetables or fruit, and a flavorful sauce or seasoning tend to feel the most satisfying all week.
How many meals should I prep for a week?
Start with two or three recipes instead of trying to prep every meal for seven days. For example, I might make one breakfast, one lunch, and one dinner or freezer backup. This keeps the prep session manageable and gives me enough variety that I am more likely to enjoy what I made.
How do I meal prep without eating the same thing every day?
Prep flexible components instead of assembling every container the same way. A cooked protein, grain or bean, roasted vegetable, salad, and sauce can be combined in different ways through the week. I also pair one portioned recipe with a make-ahead component recipe and freeze a few portions for later.
Which meals are best for meal prep lunches?
Grain bowls, hearty bean or quinoa salads, soups, chili, casseroles, and recipes with separately stored sauces are dependable lunch options. Choose recipes that travel well and follow the storage guidance on the individual recipe page, especially for salads with delicate greens or crunchy toppings.
Can I freeze meal prep recipes?
Many soups, chili, breakfast burritos, baked dishes, and some snacks freeze well, but not every meal does. Check the storage notes on the specific recipe before freezing it, cool food promptly, and label portions with the recipe name and date. Recipes with fresh greens, watery vegetables, or creamy dressings are often better prepared fresh or stored in components.
How long does meal prep last in the fridge?
Storage time depends on the recipe and its ingredients, so use the specific storage guidance on each linked recipe page. In general, I plan the week around recipes intended to be eaten first and freeze portions I will not reach promptly. When in doubt, follow standard food-safety guidance and discard anything with an off smell, appearance, or texture.
This post may contain affiliate links. Read my disclosure policy.
Stracciatella soup is a cozy Italian egg drop soup made with rich chicken broth and Parmesan. I add orzo and fresh spinach to make it a satisfying meal. Done in just 20 minutes!
Easy Stracciatella Soup Recipe
If you’ve never had stracciatella soup before, it’s an Italian version of egg drop soup. As the egg and Parmesan mixture is slowly stirred into the hot broth, it forms ribbons that give the soup its signature texture. It’s rich and full of flavor, but unlike so many other soup recipes, it comes together quickly and easily, with very little prep and cooking time. Add it to your collection of cozy chicken soups, along with Chicken Soup with Spinach and Whole Wheat Acini Di PepeandChicken and Cavatelli Soup.
Why This Stracciatella Soup Is a Favorite
I love serving stracciatella soup as a light dinner with toasted sourdough bread, but it’s also a great first course for an Italian meal. When I make it for my daughter, I leave out the spinach since she’s not a fan!
Ready in about 20 minutes: The freshly grated Parmesan and chicken bone broth add so much flavor, you don’t need a long simmer time.
Protein-packed: Eggs, Parmesan, and bone broth make this soup a good source of protein.
Comfort food meal: If chicken noodle soup is your comfort food, I have a feeling you’ll love this one too!
Ingredients You’ll Need
Below are the ingredients for this stracciatella soup. See the recipe card for exact measurements.
Reduced-sodium chicken bone broth: I like the extra nutrition bone broth offers, but regular chicken broth also works. You can swap in vegetable broth for a vegetarian stracciatella soup.
Eggs form the ribbons throughout the soup.
Freshly grated Parmesan: This is a recipe where you don’t want to use pre-grated or shredded Parmesan. You’ll notice the difference!
Fresh flat-leaf parsley adds fresh flavor.
Baby spinach wilts smoothly into the soup.
Orzo: Gluten-free orzo works too.
Freshly ground black pepper for serving.
How to Make Stracciatella Soup
You’ll find the complete instructions in the recipe card, but here’s an overview.
Mix the eggs, Parmesan, and parsley.Add the egg mixture to the broth.
Bring the broth to a boil: Heat most of the chicken broth in a large pot until boiling.
Mix the egg mixture: Whisk the remaining broth with the eggs, Parmesan, and parsley until well combined.
Cook the orzo: Add the pasta to the boiling broth and cook according to the package directions.
Create the egg ribbons: Reduce the heat to low and slowly drizzle the egg mixture into the soup while stirring.
Simmer for a minute or two.Stir in the spinach.
Finish the soup: Cook for 1 to 2 minutes, then remove from the heat. Stir in the spinach until it wilts and season with salt and black pepper to taste.
Serve: Ladle into bowls and, if desired, finish with a drizzle of olive oil, extra Parmesan, and toasted sourdough bread.
Prep: 10 minutesmins
Cook: 20 minutesmins
Total: 30 minutesmins
Yield: 6servings
Serving Size: 1cup
Bring 6 cups chicken broth to a boil.
In a medium bowl, combine remaining cup of cold chicken broth with eggs, cheese and parsley and whisk well. Set aside.
Add the orzo and cook according to package directions.
When the pasta is done, turn the heat to low and slowly drizzle the egg and cheese mixture into the pot.
Cook for 1-2 minutes, then remove from the heat, add salt as needed and black pepper to taste. Add the baby spinach and mix until it welts.
Serve in bowls with a drizzle of extra virgin olive oil (optional) and more grated cheese, if desired. Stracciatella soup is great with some toasted sourdough bread!
Last Step:
Please leave a rating and comment letting us know how you liked this recipe! This helps our business to thrive and continue providing free, high-quality recipes for you.
Stir gently: Slowly stirring creates ribbons throughout the soup. If you don’t stir enough, you’ll end up with big pieces of egg, and if you stir too much, you’ll end up with little threads of egg.
Don’t boil after adding the eggs: Keep the heat low so the eggs stay tender.
Add the Parmesan rind: If the Parmesan you buy has a rind, you can toss that in with the broth and it will add a little extra flavor to the soup. Remove it before serving.
Variations
Substitute another tiny pasta (like ditalini) for the orzo.
Add shredded rotisserie chicken for extra protein.
Serve with lemon wedges for a squeeze of brightness.
Storage and Reheating
Refrigerator: Store leftover stracciatella soup in an airtight container for up to 4 days.
To reheat: Warm gently on the stovetop or in the microwave. If the soup has thickened, you can add more broth or water when reheating.
Heart disease is a leading cause of death worldwide. But did you know that eating the right foods can help reduce your risk?
Here are the top 5 heart-healthy foods to add to your grocery list.
Salmon – Rich in omega3fatty acids, which can reduce inflammation and lower triglyceride levels.
Blueberries – Packed with antioxidants, which can help prevent the oxidation of LDL cholesterol and reduce blood pressure.
Spinach – A great source of vitamins, minerals, and fiber, which can all contribute to heart health.
Walnuts – Contains unsaturated fats and antioxidants, which can lower cholesterol and reduce inflammation
Oatmeal – High in soluble fiber, which can lower cholesterol and reduce the risk of heart disease.
By incorporating these heart-healthy foods into your diet, you can take a proactive approach to protecting your heart health
Hot peppers, soy foods, and pumpkin seeds may help with hair loss.
Androgenic or androgenetic alopecia is one of the most common chronic problems seen by dermatologists. In men, it’s called male pattern hair loss, and in women, it’s called female pattern hair loss. It’s characterized by progressive hair loss, mostly of the central scalp. I’ve talked about hair-loss supplements and hair-loss drugs; what about foods for hair loss? What role might diet play in the treatment of hair loss?
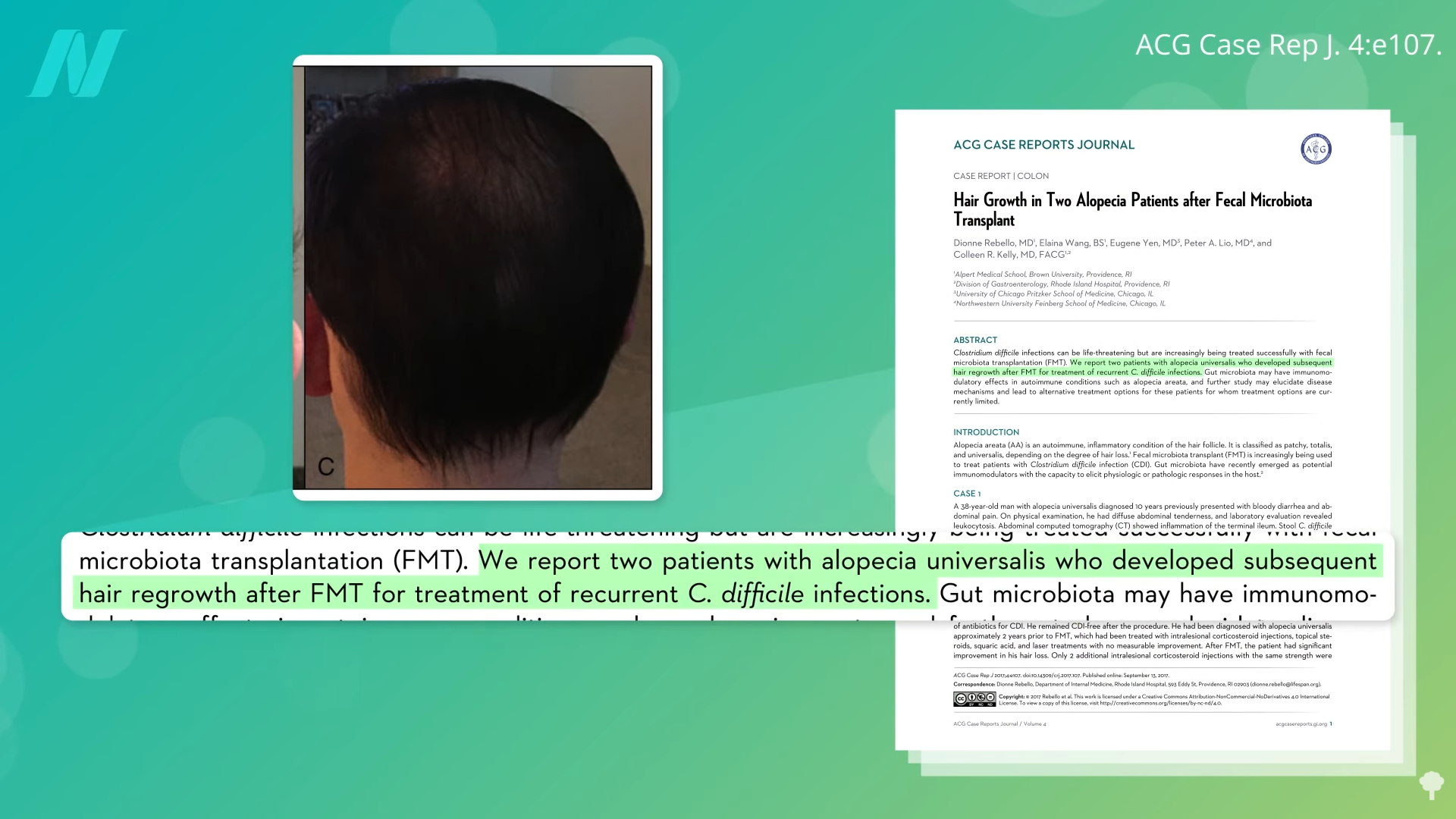
Human experiments with fecal transplants offer a clue to how powerful our microbiome is, with reports of improvements in hair loss after a “fecal slurry made from freshly passed stools” from a donor was administered into another person’s colon. These weren’t just subtle improvements. As you can see below and at 1:14 in my video Food for Hair Growth, a totally bald guy started growing back hair a few months after a fecal transplant.
A little more than a year later, his hair had completely regrown, as you can see below and at 1:18.
The moral of the story is not to drink brown smoothies, but to keep your good gut bugs happy.
Population studies have found that male pattern baldness is associated with poor sleeping habits and the consumption of meat and junk food; whereas protective associations were found for the consumption of raw vegetables and fresh herbs, as well as frequently consuming soymilk. Drinking soy beverages on a weekly basis was associated with 62% lower odds of moderate to severe hair loss, raising the possibility that there may be protective compounds in plants.
Complementary and alternative medicine treatments “boast the ability to ‘cure’ hair loss ‘safely’ with ‘less side effects’ than conventional medicine. However, it is important…to look beyond the overarching claims and marketing to critically review the literature.” For example, many studies have little relevance because the evidence was obtained from shaved rodents. (Hey, let’s smear shaved mice with bee venom!) And even when researchers do clinical studies on actual people, sometimes there’s no placebo control, so there’s no way to know if the food had anything to do with the results.
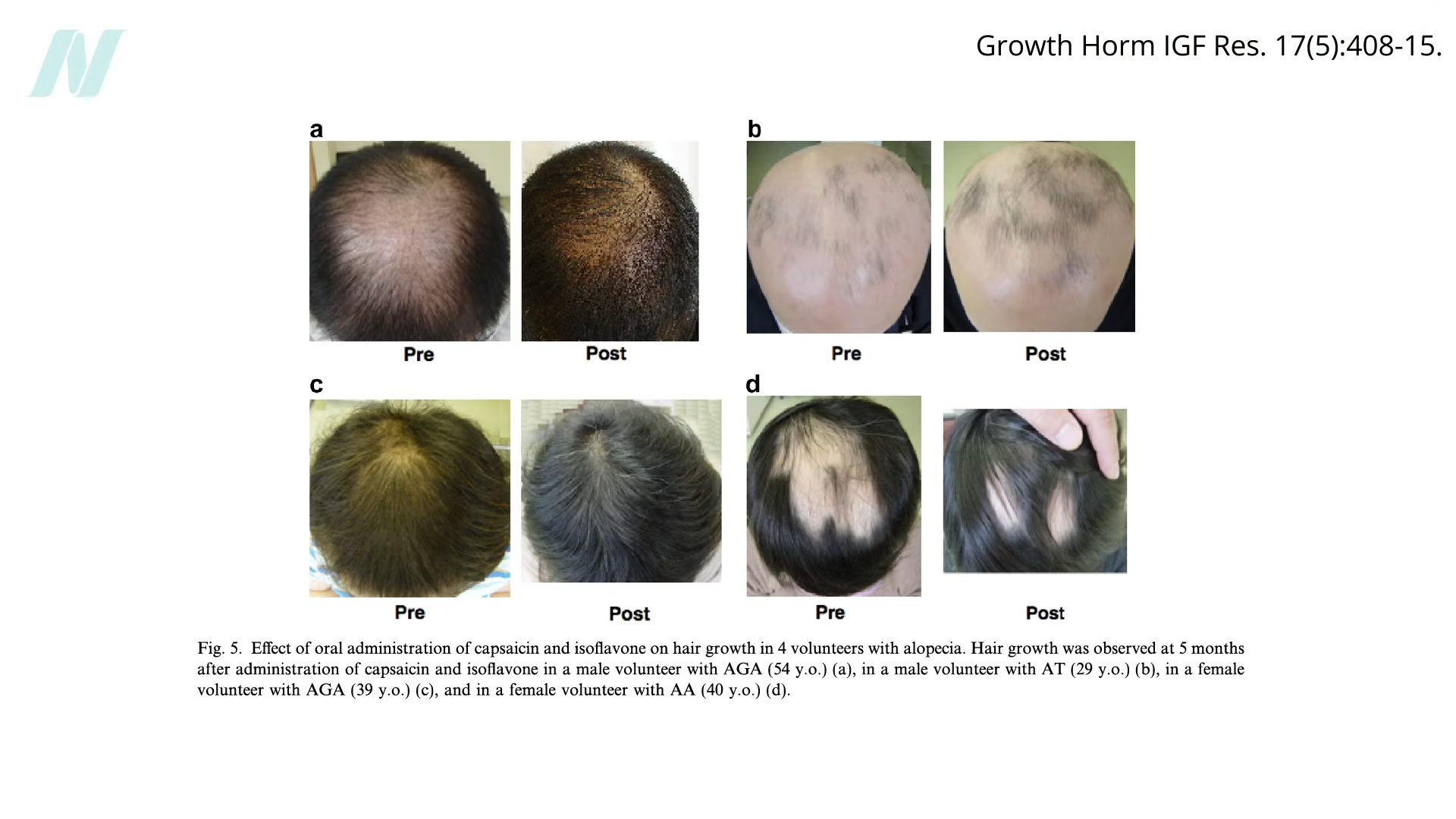
But there has been a randomized, double-blind, placebo-controlled study of compounds in hot peppers and soy, showing significantly higher promotion of hair growth. Below are some before-and-after pictures of both men and women, which you can also see at 2:49 in my video.
What doses were they taking? They took 6 milligrams of capsaicin a day and 75 milligrams of isoflavones. What does that look like in real food? You can get 6 milligrams of capsaicin in just a quarter of a fresh jalapeno pepper. That sounds pretty doable. You can get 75 milligrams of isoflavones by eating ¾ of a cup of tempeh or just straight soybeans. Soy nuts (dry-roasted soybeans) are even more concentrated, but given the formation of advanced glycation end-products in high-fat, high-protein foods prepared at high temperatures, I’d suggest avoiding routinely eating roasted or toasted nuts, seeds, or soy.
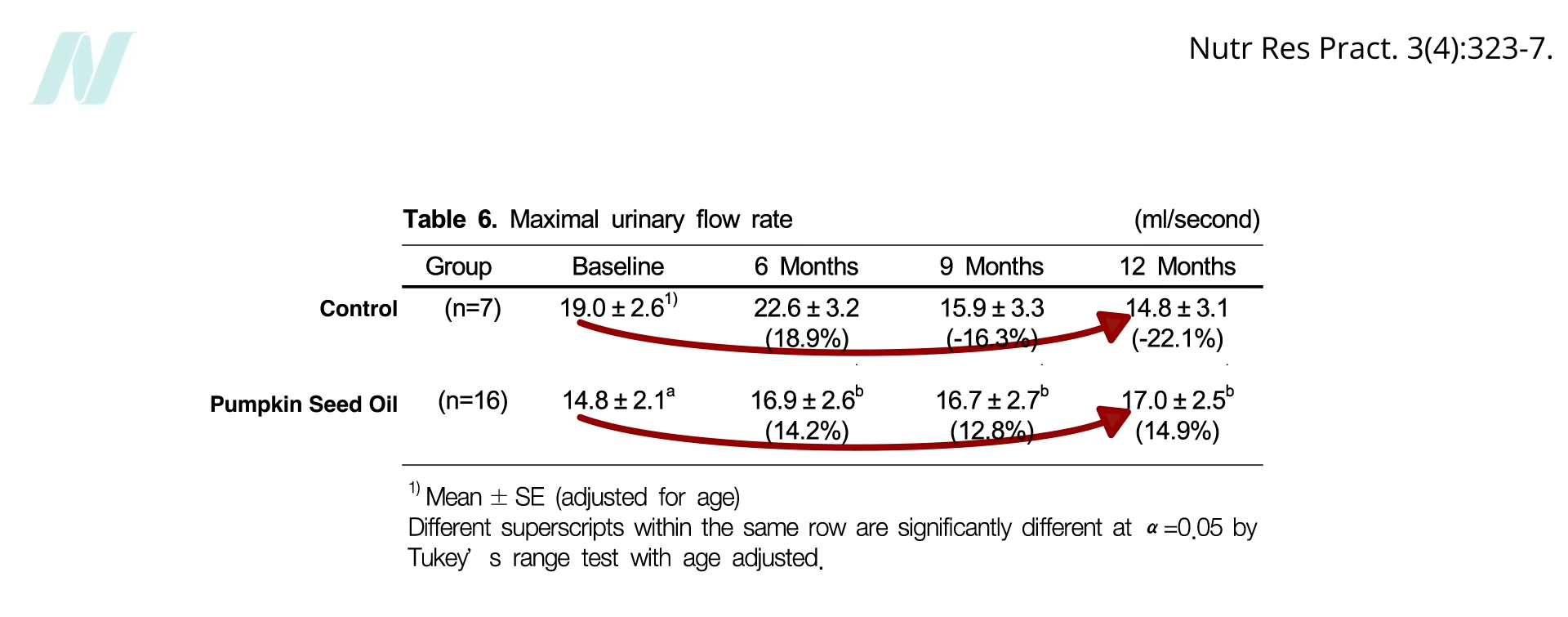
There’s also been a randomized, double-blind, placebo-controlled trial of pumpkin seed oil. Where did that idea come from? In 2009, a study out of South Korea found that randomizing men with BPH—benign prostatic hyperplasia, also known as enlarged prostate glands—to just 320 milligrams of pumpkin seed oil a day (that’s about a 16th of a teaspoon, so just a few drops a day) improved urinary flow rates. Urinary flow continued to kink off and decline in the control group, but those taking the equivalent of eating just two single pumpkin seeds a day saw a significant improvement, as you can see below and at 4:18 in my video.
That would seem to be an anti-androgen effect, so maybe it would help with hair loss. It seems to work in mice when used topically, but what about in people just eating pumpkin seeds? Sadly, we often throw away pumpkin seeds, squash seeds, watermelon seeds, and they actually have a “rich repertoire” of nutrition. But you don’t know if they actually work for hair loss until you put them to the test.
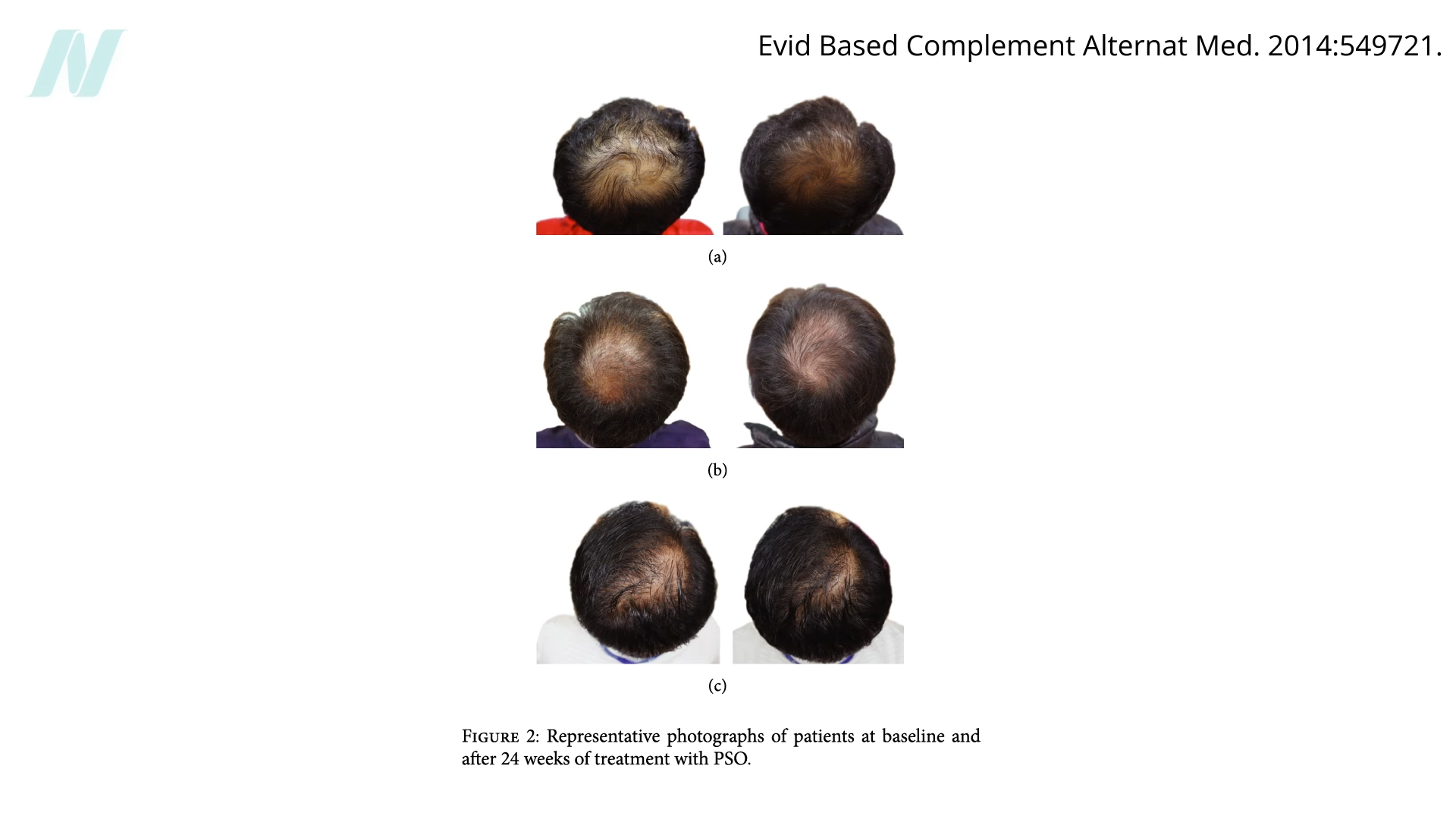
In a study, 76 men with male pattern baldness received either 400 milligrams of pumpkin seed oil a day hidden in capsules or placebo capsules for a few months. (Again, 400 milligrams is like eating two or two and a half pumpkin seeds a day.) The researchers measured scalp hair growth with all sorts of objective and subjective measures, and after 24 weeks of treatment, self-rated improvement and satisfaction scores in the pumpkin seed oil group were higher, and they objectively had more hair—a 40% increase in hair counts compared to only 10% in the placebo group. Below are some representative before-and-after shots of the improvement in hair coverage on two and a half pumpkin seeds’ worth of daily oil, which you can also see at 5:25 in my video.
Show those pictures to investigators blinded to group assignment, and they rate the placebo groups as getting slightly worse over time but the pumpkin seed oil group getting significantly better. In the pumpkin seed oil group, 95% were rated as either unchanged or improved, whereas in the placebo control group, more than 90% were classified as unchanged or worsened. Given such a pronounced effect, might we be worried about sexual side effects? Researchers used an index of erectile dysfunction before and after the study and found no evidence of adverse effects.
Doctor’s Note
This is the last in a three-part series on hair loss and growth. The previous two blogs were Do Hair Growth Supplements Work? and The Benefits and Risks of Hair Loss Drugs.
A handful of pumpkin seeds would satisfy my Daily Dozen recommendation for nuts and seeds. See Dr. Greger’s Daily Dozen Checklist.
How to Gain Weight Fast: ₹50 Diet से 3-5 Kg वजन बढ़ाएं
Hey guys! Are you tired of being skinny and looking for the best budget weight gain diet? In this video, I have shared the most affordable and effective ₹50 daily diet plan to help you gain 3 to 5 kg in just 30 days without any expensive supplements.
This video covers a complete step-by-step full day eating routine that anyone, including students and hostelers, can easily follow at home for fast muscle and weight gain results.
Topics Covered in This Video:
How to gain weight fast for skinny guys
Cheapest full day eating plan for weight gain
3-5 kg weight gain in 30 days challenge
Best budget diet plan for muscle gain
Ghar ki sasti diet se vajan kaise badhaye
If you find this video helpful, please Like, Share, and Subscribe to the channel for more fitness and diet tips!
This post may contain affiliate links. Read my disclosure policy.
This easy Creamy Pesto Pasta with cottage cheese is a great way to increase protein without adding many calories. Since it’s blended until smooth, you can’t even taste it once it’s mixed with the basil pesto.
Cottage Cheese Pesto Pasta
Since adding cottage cheese to my cottage cheese pasta sauce, I was curious how it would taste with pesto. My husband and daughter are never on board when I tell them there’s cottage cheese in anything I’m making, so I wasn’t expecting them to love this cottage cheese pesto pasta as much as they did! The cottage cheese blends seamlessly into the pesto, making the sauce extra creamy while adding extra protein. Of course, they still have no idea I added cottage cheese, and, the way I see it, they never need to know.
Why You’ll Love This Secret Ingredient
If you want to add a protein boost and achieve an ultra-smooth texture without the high calories of traditional heavy cream or excess oil, this healthy creamy pesto pasta is your new go-to.
Texture: When blended, cottage cheese transforms from curdy to silky smooth, mirroring the consistency of a high-end Alfredo sauce.
Nutrition: It turns a standard bowl of pasta into a much more satiating meal, thanks to the significant increase in protein (14.5 grams per serving!).
Ingredients You’ll Need
This simple pasta dish has 3 main components: pasta, cottage cheese, and basil pesto. Refer to the recipe card below for exact measurements.
Pasta: I used mezze rigatoni (short tubes), but any pasta shape will work.
Low-fat cottage cheese: Good Culture is my go-to since it’s thicker than most other brands.
Garlic: Use 2 or 3 cloves, depending on their size and how strong of a garlic flavor you want.
Fresh basil is my favorite herb during the summer.
Liquid: Water and olive oil help thin the sauce.
Cheese: Use Parmesan or Pecorino Romano in the pesto, and save some to grate over your pasta before serving.
Lemon juice also thins the sauce and adds bright acidity.
Kosher salt and black pepper for simple seasoning
How to Make Creamy Pesto Pasta
Don’t forget to save the pasta water! While it boils, grab a measuring cup or mug and place it by the pot as a visual reminder. The pasta water helps create a silky, smooth sauce. See the recipe card at the bottom for printable directions.
Whip the cottage cheese in the blenderMake the pestoCook pasta and stir in pesto and cottage cheese
Blend the cottage cheese and 2 tablespoons of water in a small blender until smooth.
Make the pesto: Process the garlic in a food processor, then add the basil. Once everything’s finely chopped, add the remaining water, cheese, oil, lemon juice, salt, and pepper.
Boil the pasta in a large pot of salted water, according to package directions. One minute before draining, scoop out ½ cup of pasta water. Then, drain the pasta, return it to the pot, and let it sit for a few minutes before mixing with the cottage cheese. Doing it immediately will make the cottage cheese break and become grainy.
Add the sauces: Stir the pesto into the pasta, then mix in the cottage cheese until there are no more white streaks. If it’s too thick, add a tablespoon of pasta water at a time.
How to serve: Top the pesto pasta with grated Parmesan, basil leaves, and extra salt and black pepper.
Pro Tips for the “Hidden” Texture
To ensure your family is none the wiser, follow these two simple steps:
Blend The Cottage Cheese: Use a high-speed blender or immersion blender to process the cottage cheese until it’s completely smooth before folding it into your pesto. This eliminates the “curd” texture that often makes people hesitant.
Add a splash of water or even milk to your blender when mixing the cottage cheese. This helps emulsify the sauce, creating that professional, restaurant-quality coating that clings perfectly to every noodle.
Variations
Gluten-free: You can make this dish with any type of pasta, including gluten-free or high-protein pasta.
Cottage cheese: Feel free to use whole milk cottage cheese for an even creamier sauce, but I don’t recommend fat-free because it would make the sauce too thin.
Protein boost: Add grilled chicken or shrimp.
Vegetables: Stir spinach or peas into the hot pasta.
Herbs: Try making the pesto with half basil and half parsley or chives.
Make it spicy: Sprinkle your bowl with crushed red pepper flakes.
What to Serve with Creamy Pesto Pasta
This high-protein pesto pasta can be a main dish with some vegetables on the side or a side dish with chicken, meat, or seafood.
Storage and Meal Prep Tips
Meal prep tip: Make the pesto and whipped cottage cheese a day early. Then, when it’s time to cook dinner, just boil the pasta and stir in the sauces.
Refrigerate pesto pasta for up to 4 days. If you’re packing it for lunches, store it in smaller glass containers so they’re ready to go.
Reheat: You can microwave the dish or reheat it on the stove over medium-low heat. Just don’t turn the heat up too high, or you risk the sauce curdling. If the pasta has absorbed most of the sauce, add a splash of water, milk, or broth to thin it out.
Freeze for up to 3 months; thaw in the fridge the day before.
Leftover tip: Instead of mixing the pesto cottage cheese sauce with the pasta before serving, keep the two separate and add the sauce to individual portions. That way, you won’t have to worry about the pasta soaking up the sauce.
More High-Protein Pasta Recipes You’ll Love
Looking for more ways to use cottage cheese? Check out my healthy cottage cheese recipes.
Prep: 15 minutesmins
Cook: 14 minutesmins
Total: 29 minutesmins
Serving Size: 1½ cups (scant)
Bring a large pot of generously salted water to boil.
Add the cottage cheese to a small blender with 2 tablespoons water, and process for about 15 seconds until smooth. Set aside.
Add garlic cloves to the food processor. Turn on for 15 to 30 secs until minced. Add the basil and continue processing until finely chopped. Add 3 to 4 tablespoons water, parmesan cheese, olive oil, lemon juice, salt, and pepper. Process until smooth throughout.
Once the pot is boiling, cook the pasta al dente, according to package directions. About 1 minute before draining, remove 1/2 cup pasta water and set aside. Drain the rest and pour the pasta back into the pot, remove from heat, let sit 2 minutes off the heat to prevent the sauce from breaking.
Pour in the pesto and stir, then the cottage cheese and stir well, until no streaks remain and the sauce and pasta are coated throughout.
If you would like the sauce any thinner, you may add reserved pasta water 1 tablespoon at a time until it reaches your desired consistency.
Top off with extra grated parmesan cheese, fresh basil leaves, and some extra salt and cracked black pepper, if desired.
Last Step:
Please leave a rating and comment letting us know how you liked this recipe! This helps our business to thrive and continue providing free, high-quality recipes for you.
Seasoned refried beans, salsa, and lots of melty cheese make for an epic Bean and Cheese Burrito recipe! This is one that’s all about technique and I’ll show you how to make sure your homemade burritos have the perfect golden crisp exterior and creamy filling.
You’ll never buy frozen bean burritos again!
I know the old cliché is that college students subsist entirely on ramen noodle packets, but for me, bean and cheese burritos were the other half of my diet. They were cheap, they didn’t take up much space in the freezer, and they were a pretty good source of protein.
In other words, they were good enough. But when you make your own bean burritos at home, you can go from good enough to great. Fantastic, even!
And you can pop them in the freezer for your own DIY frozen bean and cheese burritos. (My Vegetarian Burritos and Beef Burritos are great for freezing too.)
There are a few tricks that I’ll share with you as we go along, but I found that the big game-changer was making my own refried beans instead of relying on the canned version. Not only is the flavor better, but the texture is on point too—perfectly creamy rather than pasty.
Oh, and don’t skip toasting the burritos in the skillet at the end! I think the contrast between the crispy outside and the creamy inside is what makes these burritos the best.
Ingredients and Substitutions
You’ll find the full list of ingredients in the recipe card below, but here are some notes to keep in mind.
Canola Oil. Avocado oil or another neutral cooking oil works just as well.
Yellow Onion. Dice the onion into evenly-sized pieces so they all cook at the same rate.
Seasonings. Kosher salt, garlic powder, ground cumin, and black pepper give the beans some Tex-Mex flair.
Pinto Beans. Pinto beans become especially creamy when mashed or pureed, making them an excellent choice for our refried beans (which, despite their name, are not even fried once, let alone twice).
Prepared Salsa. I prefer a smooth, restaurant-style salsa because it disappears into the beans and creates a more cohesive filling. Chunky salsa works too if you want a little more texture.
Sharp Cheddar Cheese. Okay, sharp cheddar isn’t exactly authentic Mexican cheese, but I appreciate the more assertive flavor with the bean filling. Monterey Jack also works if you want something milder.
Flour Tortillas. Large 9- to 10-inch tortillas are best; they often (helpfully!) say “burrito size” on the packaging.
Nonstick Spray or Butter. For crisping the burritos. I like butter because it adds a little flavor too.
Step-By-Step Instructions
Cook the Onion (photo 1). Heat the oil in a large skillet over medium-low heat. Add the onion and cook for about 8 minutes, stirring occasionally, until it’s softened and beginning to turn golden.
Build the Filling (photo 2). Stir in the seasonings and cook for 30 seconds, or until the spices are fragrant. Add a can of pinto beans with the liquid; drain and rinse the second can, then add it along with the water and salsa. Bring to a simmer.
Mash the Beans (photo 3). Using a potato masher or the back of a wooden spoon, mash the beans until they’re as smooth or chunky as you like. Continue simmering for about 10 minutes, stirring often, until the beans are thickened but still creamy.
Warm the Tortillas. Stack the tortillas on a plate. Cover with a lightly damp paper towel and microwave for about 30 seconds. Warm tortillas are more pliable and less likely to crack.
Assemble. Sprinkle about 2 heaping tablespoons of cheese down the center of each tortilla. Top with about ½ cup bean filling and 2 tablespoons of cheese (photo 4). Fold in the short sides first, then roll tightly from one long side to the other (photo 5).
Crisp the Burritos (photo 6). Heat a nonstick skillet over medium heat. Lightly coat with nonstick spray or melt a small amount of butter. Place the burrito seam-side down. Cook for 1 to 2 minutes per side, until golden brown and crisp. Cool slightly, then slice and ENJOY!
Erin’s Testing Notes
I was trying to make the beans super creamy and the secret ended up being leaving one of the cans of beans undrained. The liquid gives the filling a satisfying richness, without the need for any additional ingredients.
I personally prefer a smooth restaurant style salsa for this recipe (as opposed to a chunky salsa) because it disappears into the beans, but it’s all personal preference.
What to Serve with Bean and Cheese Burritos
Dipping and Topping Options. Like sour cream, Guacamole, Salsa Roja, and Cilantro Lime Crema.
Rice. Cilantro Lime Rice would be perfect!
Salad. This Mexican Street Corn Salad is always a crowd-pleaser.
Bean and cheese burritos are filled with creamy beans and melty cheese, then crisped until golden for an easy, satisfying meal.
Course Dinner, Main Course
Cuisine Mexican
Prep Time 15 minutesminutes
Cook Time 20 minutesminutes
Total Time 35 minutesminutes
Servings 6burritos
Calories 407kcal
Author Erin Clarke / Well Plated
Ingredients
1 ½tablespoonscanola oilor similar neutral cooking oil
½cupyellow oniondiced
½teaspoonkosher salt
¼teaspoongarlic powder
¼teaspoonground cumin
¼teaspoonground black pepper
215-ounce cans pinto beans
½cupwater
⅔cupprepared salsaplus additional for serving
2cupsshredded sharp cheddar cheeseor Monterey Jack
6large flour tortillas9- to 10-inches
Nonstick sprayor butter, for crisping the burritos
Instructions
In a large skillet, heat the oil over medium-low. Sauté the onion until softened and turning golden, about 8 minutes.
Stir in the salt, garlic powder, cumin, and black pepper, coating the onions.
Add one can of pinto beans with its liquid. Rinse and drain the second can of beans, then add to the pan. Add the water and salsa.
Bring to a simmer over medium-high heat. With a potato masher or the back or a large spoon, lightly mash the beans and stir, leaving them as smooth or chunky as you like. Continue simmering, stirring often to prevent sticking, until the beans are thickened but spreadable, about 10 minutes. Taste and adjust the seasoning as you like.
To make the tortillas easier to roll, stack them on a plate, cover with a lightly damp paper towel, and microwave for 30 seconds.
Assemble the burritos: Down the center of each tortilla, sprinkle a 2 heaping tablespoons of cheese so it forms a line. Top with one-sixth of the mashed beans (about 1/2 cup). Add another 2 heaping tablespoons cheese on top. Fold the short sides of the tortillas over the filling to seal the ends, then lift one of the long sides up and over the filling, rolling to seal. Repeat with the remaining burritos.
When ready to eat, warm a medium nonstick skillet over medium heat. Lightly mist with nonstick spray (or melt a little butter in the skillet). Place a burrito in the skillet seamside down. Cook on each side until golden, 1 to 2 minutes per side. Let cool a few minutes, then slice and serve.
Notes
TO STORE: Wrap leftover burritos individually and refrigerate for up to 4 days.
TO FREEZE: Wrap each burrito tightly in foil or plastic wrap, then place in a freezer-safe bag for up to 3 months.
TO REHEAT: For the crispiest tortilla, warm thawed burritos in a skillet over medium heat until heated through. You can also microwave them for convenience, then finish them in the skillet for a minute or two if you’d like the outside crisp.











































































")